
The management of Hodgkin and non-Hodgkin lymphoma is often with a combination of chemotherapy and radiation. Unfortunately, due to the young age at diagnosis and high cure rates, long-term side effects in lymphoma survivors, from their initial treatment, can present a problem. Often, many oncologists will forego the best curative therapy that includes radiation therapy, because of their concern about long-term side effects from radiation that can occur decades after treatment. The side effects that are most concerning are risk of subsequent cancers and cardiovascular problems, including heart attacks and strokes.
Treating Hodgkin Lymphoma and Non-Hodgkin Lymphoma with Proton Therapy
Proton therapy can reduce the body dose of radiation by 40-50% compared with X-rays.
Modern radiation treatments in lymphoma use lower radiation doses, smaller radiation fields, and new radiation technology, such as proton therapy, which can reduce the body dose of radiation by 40-50% compared with X-rays. Proton therapy is an alternative form of radiation that is different from traditional high-energy X-ray radiation (or photons). Due to proton therapy’s unique properties, it can deliver the radiation dose to a specific depth in the body and then stop. X-ray radiation, on the other hand, continues to penetrate through normal tissue and organs (such as the lungs, heart, esophagus, breasts, and spinal cord), causing damage and toxicity.
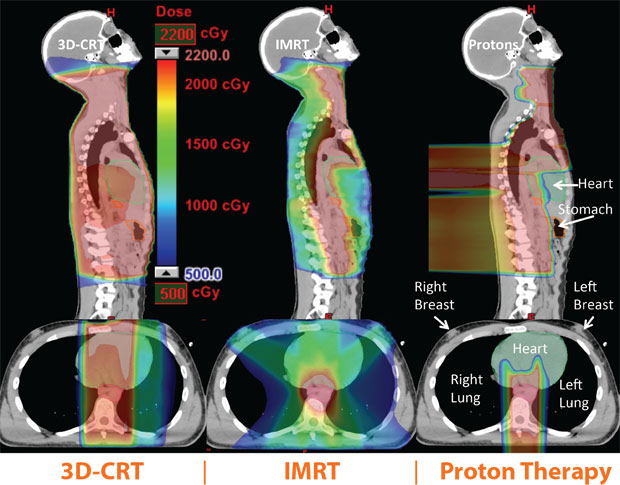
Here are some CT images that illustrate radiation exposure for the same patient with a 3D Conformal Radiation Therapy (CRT) X-ray plan (left), an intensity-modulated X-ray radiotherapy (IMRT) plan (center), and a proton therapy plan (right). The top images are sagital cuts (side view), while the bottom are transverse images (crosswise view). The color wash represents high radiation doses in red, medium doses in yellow and green, and low doses in blue. As you can see, for this patient, the proton plan substantially reduces the radiation dose to the lung (the black area in the chest), heart (green), breasts, and stomach (orange). For this patient, proton therapy is expected to reduce the risk of breast cancer, lung cancer, stomach cancer, and heart problems.
What are the clinical results of using proton therapy in patients?
University of Florida Health Proton Therapy Institute has published outcomes on using proton therapy in Hodgkin lymphoma patients and in non Hodgkin lymphoma patients.1,2 As expected, the cure rates are similar to those expected with X-ray therapy. The full benefits of using proton therapy rather than X-ray therapy are not expected to emerge until 10-20 years from now, when the late toxicities from radiation may develop, including heart problems and radiation-induced cancers.
Massachusetts General Hospital (MGH), however, has published outcomes comparing proton patients treated at their hospital for various cancers compared with X-ray patients treated on a national cancer registry, and demonstrated a 50% reduction in secondary cancers among patients getting proton therapy.3 This supports the use of proton therapy among lymphoma patients expected to live decades longer.
Which lymphoma patients benefit from proton therapy?
University of Florida Health Proton Therapy Institute conducted the first trial using proton therapy in Hodgkin lymphoma patients with involvement of the mediastinum (middle of the chest). In this study, proton therapy was able to reduce the radiation dose to all the organs at risk, including the heart, lung, breast, esophagus, and stomach compared with X-ray radiation. There was a benefit seen in using proton therapy in all patients enrolled in the study. Cure rates were similar to that seen with X-ray radiation.
In the coming decades, we expect to see survivors who have lower rates of heart problems and fewer radiation-induced cancers because proton therapy reduces the radiation dose to surrounding healthy organs.1,4,5
Proton therapy has also been shown to reduce the radiation dose to critical organs for locations in the abdomen, pelvis, and head and neck region. 6,7
Additional Support:
The National Comprehensive Cancer Network (NCCN) lymphoma guidelines committee supports the use of the radiation treatment that can best spare the organs at risk in lymphoma patients, including if that treatment modality is proton therapy.
References:
1 Hoppe BS, Flampouri S, Zaiden R, Slayton W, Sandler E, Ozdimir S, Dang N, Li Z, Morris C, Mendenhall NP. Involved-node proton therapy in combined-modality therapy for Hodgkin lymphoma: results of a Phase II study. Int J Radiat Oncol Biol Phys. 2014;89(5):1053-1059.
2 Sachsman S, Flampouri S, Li Z, Lynch J, Mendenhall NP, Hoppe BS. Proton therapy in the management of non-Hodgkin lymphoma. Leukemia & Lymphoma. 2015;11:1-20 [Epub ahead of print].
3 Chung CS, Yock TI, Nelson K, Xu Y, Keating NL, Tarbell NJ. Incidence of second malignancies among patients treated with proton versus photon radiation. Int J Radiat Oncol Biol Phys. 2013;87(1):46-52.
4 Hoppe BS, Flampouri S, Su Z, Morris CG, Latif N, Dang NH, Lynch J, Li Z, Mendenhall NP. Consolidative involved-node proton therapy for Stage IA-IIIB mediastinal Hodgkin lymphoma: preliminary dosimetric outcomes from a Phase II study. Int J Radiat Oncol Biol Phys. 2012;83(1):260-267.
5 Hoppe BS, Flampouri S, Su Z, Latif N, Dang NH, Lynch J, Joyce M, Sandler E, Li Z, Mendenhall NP. Effective dose reduction to cardiac structures using protons compared with 3DCRT and IMRT in mediastinal Hodgkin lymphoma. Int J Radiat Oncol Biol Phys. 2012;84(2):449-455.
6 Sachsman S, Hoppe BS, Mendenhall NP, Holtzman A, Li Z, Slayton W, Joyce M, Sandler E, Flampouri S. Proton therapy to the subdiaphragmatic region in the management of patients with Hodgkin lymphoma. Leukemia & Lymphoma. 2014 Nov [Epub ahead of print].
7 Maraldo MV, Brodin NP, Aznar MC, Vogelius IR, Munck Af Rosenschöld P, Petersen PM, Specht L. Doses to the head and neck normal tissues for early stage Hodgkin lymphoma after involved node radiotherapy. Radiother Oncol. 2014;110(3):441-447.
Additional Readings:
Li J, Dabaja B, Reed V, Allen PK, Cai H, Amin MV, Garcia JA, Cox JD. Rationale for and preliminary results of proton beam therapy for mediastinal lymphoma. Int J Radiat Oncol Biol Phys. 2011;81(1):167-174.
Holtzman A, Hoppe BS, Li Z, Slayton W, Sandler E, Joyce M, Ozdemir S, Mendenhall NP, Flampouri S. Advancing the therapeutic index of pediatric patients with Stage III Hodgkin lymphoma with proton therapy. Int J of Particle Therapy. 2014;1(2):343-356.
Figura N, Flampouri S, Hopper K, Marcus R, Mendenhall NP, Hoppe BS. Consolidative proton therapy following high-dose chemotherapy and autologous stem cell transplant in an adolescent with relapsed Hodgkin lymphoma. JAYAO. 2011;1(2):103-106.
Hoppe BS, Flampouri S, Li Z, Mendenhall N. Cardiac sparing with proton therapy in consolidative radiation therapy for Hodgkin lymphoma. Leukemia & Lymphoma. 2010;51(8):1397-1398.
Rutenberg MS, Flampouri S, Hoppe BS. Proton therapy for Hodgkin lymphoma. Current Hematologic Malignancy Reports. 2014;9(3):203-211.
Ho CK, Flampouri S, Hoppe BS. Proton therapy in the management of lymphoma. The Cancer Journal. 2014;20(6):387-392.
Hoppe BS, Flampouri S, Lynch J, Slayton W, Zaiden R, Li Z, Mendenhall NP. Improving the therapeutic ratio in Hodgkin lymphoma through the use of proton therapy. Oncology. 2012;26(5):456-465.
Survivor Spotlights

Cancer Treatment Specialist(s)

